
Introduction
Pharmaceutical and biotech manufacturers face a structural tension that gets more acute every year. FDA approved 50 novel drugs in 2024, and PhRMA reports over 2,000 cell and gene therapies currently in clinical development — yet the facilities required to manufacture these therapies are capital-intensive, long-lived assets designed years before commercial demand is confirmed.
Traditional "build-once" pharma facilities lock in infrastructure at the worst possible moment: before you know which products will succeed, what scale you'll need, or what regulatory expectations will look like five years from now.
Modular pharma facility design treats adaptability as a design requirement, not an afterthought. When approached as a design philosophy — not just a procurement or construction method — it embeds flexibility into the facility's structure from the start.
This post covers:
- What makes modular design future-proof (and what doesn't)
- How to plan for scalable, phased growth
- Where GMP compliance and validation fit the modular model
- Which planning decisions matter most before a single module is fabricated
Key Takeaways
- Modular pharma facility design is a design philosophy centered on interoperability, replaceability, and adaptability — not just off-site fabrication
- Future-proof facilities require standardized interfaces, utility spine architecture, and flexible HVAC/cleanroom classification from day one
- ISPE reports modular construction can compress project timelines by up to 50% through parallel off-site fabrication
- Factory-controlled fabrication improves GMP compliance through tighter quality control and pre-structured documentation packages
- Early, integrated multi-discipline coordination is the single most critical success factor
What Is Modular Pharma Facility Design?
Modular pharma facility design is an approach in which discrete, pre-engineered building systems and process units are designed with standardized interfaces and off-site fabrication in mind, then integrated into a coherent facility.
The components typically designed as modules include:
- Cleanroom envelope systems — wall, ceiling, and floor assemblies pre-configured for specific ISO classifications
- HVAC and utility skids — clean steam, purified water, compressed gases, and air handling units assembled off-site
- Process equipment assemblies — skid-mounted bioreactor systems, fill/finish equipment rooms, and buffer preparation units
- Automation and control panels — pre-wired, pre-programmed panels that integrate into facility SCADA/DCS architecture
The degree of modularization runs a wide spectrum — from partial (utility skids only) to near-complete (pre-validated production suites). ISPE defines modular manufacturing facilities as those that assemble prefabricated sub-assemblies in controlled factory settings to create substantially complete manufacturing units.
More Than a Construction Method
The deeper distinction is at the design phase, not the construction site. Future-proofing begins with how a facility is designed: standardized module interfaces, utility spine architecture, and zoning strategies that anticipate change.
BioPhorum frames this as a standardized approach for multi-product biopharmaceutical manufacturing — one that accelerates project lifecycles and supports multiple complex products across a facility's operational life.
That distinction matters in practice. A facility that uses prefabricated components but wasn't designed for interchangeability can't be meaningfully reconfigured later. True modular design specifies every connection point, utility supply route, and cleanroom zone with future change in mind — so modifications that would otherwise require demolition become planned-for reconfigurations instead.
Core Design Principles for a Future-Proof Modular Facility
Five design principles separate modular facilities that remain adaptable over decades from those that become rigid after the first expansion.
Principle 1: Standardized Interfaces Between Modules
When modules can't be swapped cleanly, the whole system stalls. Avoiding that outcome requires clearly defined, standardized connection points — mechanical, electrical, controls, and structural — so individual units can be upgraded without disrupting adjacent systems.
This demands upfront alignment across architecture, MEP, and process disciplines. Interface definitions finalized late — or left to construction teams — are the most common source of costly rework.
Key interface requirements to lock down during design:
- Mechanical connection standards (pipe sizes, flanges, utility stub locations)
- Electrical and controls termination points per module boundary
- Structural load ratings at every inter-module junction
- Data/network handoff protocols between adjacent zones
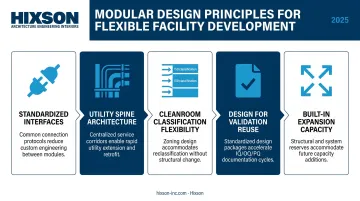
Principle 2: Utility Spine Architecture
A central utility corridor or "spine" supplies HVAC, purified water, clean steam, electrical power, and data infrastructure to production modules. This architectural strategy means production zones can be modified or reconfigured without rebuilding utility infrastructure. Underground utility corridors and raised flooring systems are two common implementations — both keep service routes accessible and expandable without disrupting active production areas.
Principle 3: Cleanroom Classification Flexibility
Designing HVAC systems, wall and ceiling envelope systems, and airlock configurations to accommodate multiple ISO classifications gives facilities the ability to shift production types — from small molecule to biologics, for example — without full reconstruction. EU GMP Annex 1's requirement for a documented Contamination Control Strategy means this flexibility must be designed and validated, not assumed.
Principle 4: Design for Validation Reuse
Standardized, repeatable module designs support a library of pre-qualified configurations — which means faster IQ/OQ/PQ activities when modules are replaced or added. EU GMP Annex 15 confirms that qualification principles apply to facilities, equipment, and utilities, with FAT/SAT concepts embedded in the lifecycle.
What makes validation reuse credible under regulatory scrutiny:
- Documentation protocols established during design, not retrofitted post-construction
- Design standards that mirror previously qualified configurations
- FAT/SAT protocols aligned to modular boundaries from the start
Principle 5: Built-In Expansion Capacity
Structural load capacity, utility headroom, and space adjacencies must anticipate future module additions from the start. Hixson's pharma master planning services address this — covering future cleanroom expansion, clean utility infrastructure, and phased capital deployment aligned with pipeline progression. A practical benchmark: size utility infrastructure for 150% of current projected load, and confirm structural bays can accept additional modules without shoring or re-engineering.
Scalability and Phased Growth: Designing for What Comes Next
Phased Capital Deployment
Modular design allows manufacturers to begin with a core production footprint and add modules as commercial demand confirms it. This aligns capital expenditure with pipeline milestones and reduces financial exposure during uncertain development phases.
Hixson's pharma and biotech master planning approach reflects this directly — incorporating visioning sessions with senior leadership, manufacturing capacity analysis, phasing plans, and cost estimates that build flexibility into the original site plan rather than treating expansion as a future problem.
For greenfield projects, the master plan lays out the site to support sequential module additions. For brownfield expansions, modules can be pre-fabricated and pre-tested off-site, then installed during a compressed on-site window — keeping disruption to operating facilities to a minimum.
Hixson's work with Unither Pharmaceuticals illustrates this thinking: a facility designed with strategic space for two additional manufacturing lines from the outset, rather than retrofitting for growth after the fact.
Timeline Advantages
ISPE data puts the schedule advantage in concrete terms: modular construction can reduce program durations by up to 50% when off-site building manufacture overlaps with site preparation. Modular bioprocess facilities can be fully operational in 18–24 months — roughly half the timeline of a comparable conventional build.
Product Changeover and Multi-Product Flexibility
Biologics, cell and gene therapy, and specialty drug manufacturers face a specific challenge: multiple products, evolving campaigns, and the need to reconfigure production suites without extended downtime. Modular production suites designed for rapid reconfiguration — including single-use technology compatibility and segregated airlock systems — reduce changeover time between campaigns.
No public benchmark data currently exists comparing precise changeover timelines in modular versus traditional facilities, but the design drivers are consistent:
- Pre-defined airlock transitions that standardize suite entry and exit protocols
- Standardized utility connections that simplify reconfiguration between product campaigns
- Single-use systems that eliminate dedicated cleaning validation between runs
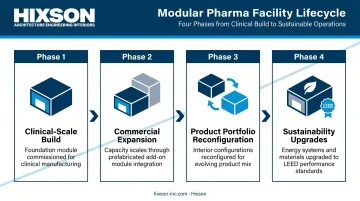
Lifecycle and Sustainability Alignment
Modular design supports the full facility lifecycle — from clinical-scale manufacturing through commercial-scale production — without requiring a new facility build at each stage. Modules can be added, reconfigured, or retired as the product portfolio evolves.
That same replaceability is what connects modular design to sustainability goals. ISPE's guidance on environmental sustainability in biopharmaceutical facility design calls for science-based analyses of environmental impacts from materials, processes, and architecture. Swapping an HVAC module for a more energy-efficient unit as technology improves supports LEED-aligned design strategies — without requiring full facility reconstruction.
GMP Compliance and Validation in Modular Design
Factory-Controlled Fabrication and IQ Documentation
Controlled fabrication environments reduce construction variation, contamination risk during build, and rework during commissioning. Documentation of build quality — materials, welds, surface finishes — can be completed before modules arrive on site, directly supporting Installation Qualification activities.
Under 21 CFR 211.42, manufacturing buildings must be of suitable size, construction, and location. Factory-controlled fabrication gives design teams a reliable path to meeting that standard consistently across multiple modules. Pre-arrival documentation packages give quality teams a cleaner starting point for site-based qualification — typically covering:
- As-built conditions
- Material certificates
- Weld inspection records
Structured CQV Advantages
Modular design creates opportunities to structure commissioning, qualification, and validation activities differently than in traditional builds:
- Factory Acceptance Testing (FAT) can be conducted at the fabrication facility, resolving issues before shipping
- Site Acceptance Testing (SAT) focuses on integration and interface verification rather than system-level commissioning from scratch
- On-site validation timelines compress because substantial qualification evidence already exists from the FAT package
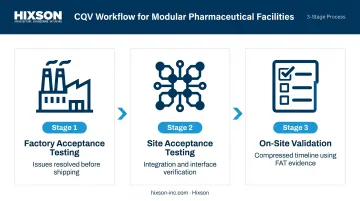
EU GMP Annex 15 includes FAT and SAT as explicit components of the qualification lifecycle. The key constraint is that FAT evidence doesn't eliminate on-site qualification — it accelerates it by reducing discovery work. Engage CQV planning teams at the design stage, not after construction begins, so that module documentation requirements are designed in rather than retrofitted.
Module-to-Module Interface Risk
Even with structured CQV, the physical connections between modules are where risk re-emerges. Seams, utility connections, and integration points require careful design and validation attention. These are common sites for contamination risk, airflow anomalies, and utility discrepancies — and they are design-phase issues, not construction-phase issues. EU GMP Annex 1's Contamination Control Strategy requirement means every interface must be analyzed and addressed in the CCS documentation, not discovered during commissioning.
Planning and Implementation Considerations
The Most Critical Success Factor
Early, integrated coordination between architecture, process engineering, MEP, controls, and quality/regulatory teams separates successful modular pharma projects from costly ones. When disciplines work sequentially, the benefits of modular design erode quickly.
Interface misalignments, utility conflicts, and validation gaps are most often the product of late-stage coordination — not inherent limitations of the modular approach itself.
Firms with deep in-house multi-discipline capability reduce this risk by design. Hixson's 20 integrated technical disciplines operate from the same project model rather than passing information across organizational boundaries. Those disciplines include:
- Architecture, civil, and structural engineering
- Mechanical, electrical, and plumbing (MEP) systems
- Process engineering and controls & automation
- Commissioning, qualification, and validation (CQV) support

Key Early-Stage Planning Decisions
These decisions must be resolved before detailed design begins:
- Module sizing relative to transport constraints — federal limits of 102-inch width and 80,000 lb gross weight define the physical envelope; state oversize permits are required for anything larger
- Site logistics — crane access, laydown areas, sequencing of module installation, and temporary utility connections during phased builds
- Utility connection standards — defining standardized connection types and sizes across all modules so that future additions don't require custom interfaces
- Change control protocols — establishing how module modifications are documented and controlled within the facility's quality management system
Pitfalls to Avoid
The most common and costly mistakes in modular pharma facility projects:
- Under-designing structural and utility headroom for future expansion — remediation after construction is expensive; upfront allowances cost a fraction of that
- Treating modular design as a procurement decision rather than a design philosophy — purchasing prefabricated components for a facility not designed for interoperability captures only a fraction of the potential value
- Failing to involve CQV planning early — module documentation requirements that aren't established during the design phase create validation gaps that delay occupancy and regulatory submissions
Frequently Asked Questions
What types of pharmaceutical facilities benefit most from modular design?
Biologics manufacturers, cell and gene therapy producers, CMOs, and any manufacturer with multiple products or evolving pipelines are strong candidates. Modular design delivers the most value when future adaptability is a strategic priority, not an afterthought.
How does modular pharma facility design support GMP compliance?
Factory-controlled fabrication environments improve build consistency and produce traceable documentation that supports Installation Qualification. Standardized module configurations can underpin pre-qualified designs, reducing on-site commissioning time and providing a clear audit trail during regulatory inspections.
What is the difference between modular and traditional pharma facility construction?
Traditional construction is sequential and site-built; modular construction runs fabrication in parallel with site preparation. The deeper difference is design philosophy — modular design prioritizes interoperability, standardized interfaces, and future adaptability from the earliest planning stage.
How long does it typically take to complete a modular pharmaceutical facility?
According to ISPE, modular construction can reduce program durations by up to 50% compared to traditional builds. Industry references for modular biomanufacturing facilities cite timelines of 18–24 months from project start to operational readiness.
Can an existing pharmaceutical facility be expanded using a modular approach?
Yes — brownfield modular expansion is one of the most common applications. Teams pre-fabricate and test modules off-site, then install them during planned production windows to minimize disruption to ongoing manufacturing operations.
What are the biggest design challenges in modular pharma facility projects?
Early interface definition between modules, transport and site logistics constraints, and multi-discipline coordination are the primary challenges. All three are most effectively managed when architecture, MEP, process, controls, and quality teams are engaged from the master planning stage forward.


