Introduction
BSL-3 laboratories are specialized containment facilities designed to study infectious agents that may be transmitted through the air and cause potentially lethal infections. Getting the design right isn't optional — it's a direct determinant of researcher safety, regulatory compliance, and whether the facility passes certification before first occupancy.
This guide is written for architects, engineers, facility planners, and institutional administrators planning to build, renovate, or commission a BSL-3 lab. The stakes here are different from standard laboratory work. A missed penetration seal, a misdirected door swing, or an HVAC system that reverses pressure under failure conditions aren't just construction defects — they're containment failures.
This guide covers:
- The regulatory framework governing BSL-3 design
- Physical and engineering requirements for a compliant facility
- The design process from pre-planning through annual recertification
- Common mistakes that derail these projects
Key Takeaways
- BSL-3 labs handle pathogens with serious airborne transmission risk — design must address that hazard at every level, from envelope sealing to HVAC failure modes
- Key governing documents: CDC/NIH BMBL 6th Edition, NIH Design Requirements Manual (Rev. 1.5), and ANSI/ASSP Z9.14-2020
- Required design features: two interlocked self-closing doors, inward directional airflow, non-recirculated exhaust, sealed envelope, and a hands-free sink near the exit
- Architecture, mechanical, electrical, biosafety, and end-user teams must collaborate from day one — not after design is locked
- Annual recertification is mandatory; design decisions made now determine how expensive and difficult that process will be every year
What Is a BSL-3 Laboratory?
BSL-3 is the third of four biosafety levels defined by the CDC and NIH. Per the BMBL 6th Edition, it applies to work with indigenous or exotic agents that may cause serious or potentially lethal disease through the inhalation route — pathogens such as Mycobacterium tuberculosis, Coxiella burnetii, and St. Louis encephalitis virus.
Where BSL-3 Sits in the Framework
BSL-3 builds on every requirement established at BSL-1 and BSL-2, then adds a substantially more demanding layer of engineering controls and physical containment. The key distinction from BSL-2 is the inhalation hazard: BSL-2 addresses agents transmitted through ingestion, percutaneous exposure, or mucous membrane contact. BSL-3 adds aerosol containment as the core design driver.
BSL-4 sits above it, reserved for agents with high aerosol transmission risk and no available vaccines or treatments. It requires either a Class III cabinet system or full-body air-supplied positive pressure suits — containment rarely needed outside a handful of national biocontainment facilities.
Understanding where BSL-3 sits between these levels also shapes how designers approach facilities that may not yet need full BSL-3 operations but need to be built for them.
The BSL-2+ Strategy
The BSL-2+ facility is a lab built to BSL-3 physical specifications but operated under BSL-2 protocols. This allows institutions to conduct current research at BSL-2 while preserving the option to upgrade if research needs change.
It's an increasingly common strategy in new construction — particularly for institutions with long-term roadmaps that may involve emerging pathogens. The key is committing to BSL-3 architectural and mechanical design standards from the start, even if full BSL-3 operations aren't anticipated immediately.
BSL-3 Laboratory Design Requirements: Physical Space and Architecture
Primary Containment: Biosafety Cabinets and PPE
All manipulations of infectious materials in a BSL-3 lab must be conducted inside a certified biosafety cabinet (BSC) or equivalent containment device. The choice of cabinet type has direct implications for exhaust system design:
- Class II Type A2 cabinets recirculate a portion of cabinet air and exhaust the remainder. They can be connected to building exhaust via a canopy connection, but don't require a hard-duct connection
- Class II Type B2 cabinets exhaust 100% of cabinet air and require a dedicated hard-duct exhaust connection, which directly increases exhaust fan sizing requirements and affects the entire HVAC design
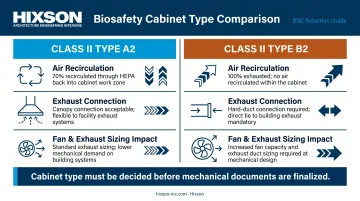
Upgrading from Type A2 to Type B2 mid-design without recalculating exhaust fan curves is one of the most common engineering-phase mistakes on these projects. The decision must be made early, in coordination with the mechanical engineer — before architectural and mechanical documents diverge.
PPE requirements complement cabinet containment. Respirators may be required depending on the risk assessment. The anteroom must be designed to accommodate storage, donning and doffing areas, and dedicated charging stations where PAPRs (powered air-purifying respirators) are used.
Secondary Containment: Architectural Features
Entry sequence. BMBL requires access through two consecutive self-closing doors. The NIH Design Requirements Manual adds the requirement for interlocked anteroom doors, meaning both cannot be open simultaneously. Door swing direction relative to airflow is a critical detail that's frequently overlooked: doors should swing in the direction that supports containment — swinging against airflow creates a pressure gap that can compromise the containment envelope.
Sealed envelope. Every window must be sealed and inoperable. All penetrations through walls, floors, and ceilings (for conduit, piping, and ductwork) must be sealed with non-shrink, corrosion-resistant, gastight permanent sealants. The NIH DRM requires penetrating components to be braced to maintain seal integrity over time.
Surfaces and finishes. Floors, walls, and ceilings must be smooth, non-porous, and impervious to liquids. They must resist the full range of chemicals and vapor-phase decontaminants used in BSL-3 environments. The NIH DRM specifies integral coved bases of at least 152mm. Wall-hung or movable casework is preferred over floor-supported units; fixed floor-supported cabinets create cleaning dead zones that are difficult to decontaminate and may fail inspection.
Access Control and Safety Fixtures
Handwashing sinks. Hands-free or automatically operated sinks are required near the lab exit. The NIH DRM specifies hard-wired electric sensors or off-the-floor foot pedals with slow-close valves. Any touchable faucet handle is non-compliant.
Eyewash stations must be positioned for immediate accessibility without requiring travel through contaminated areas.
Access control must restrict entry at all times. Electrical panels must be located outside containment. Communication devices, security cameras, and workstations must be sealed to the containment barrier to the same standard as other penetrations; open conduit paths through the envelope are a common inspection failure point.
Critical Engineering Systems in BSL-3 Labs
Directional Airflow and Pressure Differentials
The fundamental airflow principle in BSL-3 design: air must flow inward at all times, from lower-contamination areas (corridor) through the anteroom and into the lab — never the reverse. This must hold under all operating conditions, including fan failure and door-open scenarios.
Pressure differentials at each containment barrier door must be validated during commissioning and monitored continuously during operations. The NIH DRM requires visual readout devices — magnehelic gauges or digital monitors — at lab and anteroom entries so personnel can verify system performance before entering.
Three building conditions that can reverse containment airflow if not addressed in design:
- Stack effects from elevator shafts or tall atriums creating unintended pressure gradients
- Adjacent independent HVAC systems pulling air across containment boundaries
- Structural limitations that prevent the room envelope from tolerating deep negative pressure
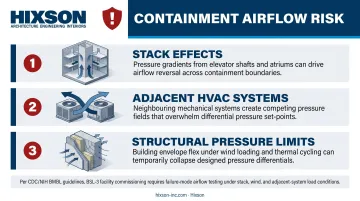
CDC policy on BSL-3/ABSL-3 verification explicitly requires that airflow must not reverse at the containment barrier under failure conditions. Testing failure scenarios — not just normal operation — is a certification requirement, not an optional commissioning step.
HEPA Filtration and Exhaust Systems
Airflow direction is only part of the containment equation. Where exhaust goes — and how it's treated — determines whether the lab can recirculate or must discharge.
BSL-3 exhaust air cannot be recirculated to any other part of the building. The BMBL frames HEPA filtration as a conditional requirement: exhaust must either be discharged away from occupied areas and air intakes, or be HEPA filtered. Which path applies depends on the risk assessment, applicable regulations, and whether the facility handles select agents.
When HEPA filtration is required, filter placement matters. The NIH DRM recommends locating exhaust HEPA filters as close as possible to the containment barrier penetration — not at a distant central location with long contaminated duct runs in between.
Central vs. room-level HEPA: the design trade-off
| Approach | Advantage | Consideration |
|---|---|---|
| Central HEPA unit | Fewer units requiring annual decontamination and testing | Higher upfront cost; single point of failure if not redundant |
| Room-level local HEPA | Shorter contaminated duct runs; modular | Multiplies annual certification costs per unit |
This decision has long-term budget implications. It should be evaluated during design with both capital and operating costs on the table.
Redundancy requirements. The NIH DRM requires N+1 redundancy for critical HVAC components, including air handlers and exhaust fans. Two exhaust fans operated together at reduced speed — rather than one running and one on standby — provide faster pressure recovery during fan failure. Pressure differential gauges at anteroom and lab entries give personnel real-time system status.
Plumbing, Decontamination, and Electrical Systems
HVAC is only one layer of a BSL-3's engineering envelope. Autoclave placement and electrical distribution introduce separate containment risks that are frequently underestimated in early design.
Autoclave placement and bioseal. BSL-3 labs require an autoclave or validated alternative decontamination method for all lab waste. Where a pass-through autoclave is used:
- The bioseal must be on the containment side of the barrier
- Master controls must be accessible from outside containment
- Effluent discharge must occur on the clean side
Treating the autoclave bioseal as a plumbing detail — rather than a containment detail — is an error that has caused costly change orders on real projects.
Electrical distribution. Circuit breakers and panels must be located outside containment, with all receptacles within containment labeled with breaker identification. Key power design requirements include:
- Dedicated emergency generator (not shared with the building's general emergency system — a shared generator is a single point of failure)
- UPS systems for room-level HVAC control components to cover the interval between power loss and generator startup
The BSL-3 Design Process: From Planning to Certification
Pre-Design Planning and Basis of Design
A well-defined Basis of Design (BOD) document is the foundation of every compliant BSL-3 project. It should specify:
- The research program's intended agents and workflows
- Equipment requirements, including BSC types and autoclave configuration
- Personnel and waste movement pathways
- Future flexibility requirements (BSL-2+ capability, potential agent upgrades)
A vague BOD means the design can't be engineered to the correct containment level — and compliance gaps discovered after construction is complete are among the most expensive problems a facility can face.
Early pathways drawings mapping personnel movement, material flow, and waste removal should be produced before any design decisions are locked in. Boundary ambiguities that take an hour to resolve on paper can require structural modifications in the field.
Integrated Design Team
BSL-3 design is not a sequential handoff from architect to engineer. It requires parallel, integrated input from day one. The team must include:
- Principal investigator and future lab users
- Biosafety officer
- Architect and interior designer
- Mechanical and electrical engineers
- A BSL-3 certifier or biosafety subject matter expert
- Facilities director and finance representative

Decisions about HEPA filtration type, emergency power scope, and decontamination configuration all carry capital and operating cost implications. They can't be made in disciplinary silos.
The coordination between airflow design, penetration sealing, equipment integration, and BAS programming is where design errors most often originate on these projects. Integrated A/E firms — where those disciplines share models and work in parallel rather than in handoff sequence — substantially reduce the gap between what's designed and what gets built. Hixson's structure, with 20 in-house technical disciplines spanning architecture, MEP, process engineering, and controls, reflects this directly.
Commissioning, Certification, and Recertification
BSL-3 labs must undergo comprehensive performance testing before first occupancy. Per BMBL, design parameters, operational procedures, and systems must be verified and documented before operation — then retested at least annually or after any significant modification.
Certification testing covers:
- Differential pressure verification under normal and failure scenarios
- Quantitative directional airflow confirmation
- HEPA filter integrity testing
- Alarm system confirmation
- Interior and exterior inspection
Design teams that treat certification criteria as a design input — not a post-construction checklist — build labs that pass the first time and avoid costly last-minute fixes.
Annual recertification is an ongoing operational cost. Design decisions that simplify it — accessible maintenance panels, properly located exhaust control valves, labeled circuit breakers, pressure gauge placement visible from outside the anteroom — matter every year for the life of the facility.
Common BSL-3 Design Pitfalls to Avoid
Incomplete Basis of Design. Failing to define the research program before design begins is the costliest early mistake. Labs without shower-out provisions, effluent decontamination plumbing, or defined personnel and waste pathways create containment boundary ambiguities — ones that surface during certification, not during design, when corrections are still inexpensive.
Mid-design equipment changes without system recalculation. Common engineering-phase mistakes include:
- Upgrading a BSC from Type A2 to Type B2 without recalculating exhaust fan curves
- Placing freezers in concentrated areas without accounting for heat loads in air distribution
- Omitting exhaust ducting over autoclave chambers
- Combining BSL-2 and BSL-3 exhaust ductwork due to misinterpretation of containment guidelines
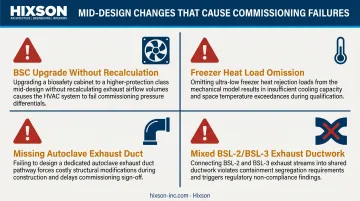
Each of these has caused failed commissioning and substantial change-order claims on real projects.
HVAC failure mode reversals. An HVAC system that reverses containment airflow under failure conditions is the most safety-critical design flaw in a BSL-3 project. Several factors can drive this failure:
- Building stack effects pulling air toward the containment zone
- Adjacent independent systems creating unintended pressure differentials
- Structural constraints that prevent achieving or sustaining deep negative pressure
Each must be accounted for during design and explicitly tested during commissioning. CFD airflow modeling during design — not field discovery during certification — is the standard for catching and mitigating these risks.
Frequently Asked Questions
What is a BSL-3 laboratory type?
BSL-3 is the third of four CDC/NIH biosafety levels, used for work with pathogens capable of causing serious or fatal disease through airborne transmission. It requires specific engineering controls, administrative procedures, and physical containment features that go substantially beyond BSL-1 and BSL-2 requirements.
What are the physical and engineering requirements for BSL-3 laboratory design?
BSL-3 design requires two self-closing interlocked entry doors, sustained inward directional airflow with 100% non-recirculated exhaust, sealed surfaces and penetrations, a hands-free sink near the exit, and all infectious work conducted inside a certified biosafety cabinet. HEPA filtration requirements are determined by the facility risk assessment, with all design decisions guided by the BMBL and NIH Design Requirements Manual.
What is the difference between BSL-3 and BSL-4 laboratories?
BSL-4 handles agents with no available vaccines or treatments that pose high aerosol transmission risk. It builds on all BSL-3 requirements, adding either a Class III cabinet line or full-body air-supplied positive pressure suits. BSL-4 facilities also require a separate building or fully isolated zone with independent HVAC.
What guidelines govern BSL-3 laboratory design in the United States?
The primary governing documents are the CDC/NIH BMBL 6th Edition, the NIH Design Requirements Manual (Rev. 1.5), and ANSI/ASSP Z9.14-2020 for ventilation system testing and performance verification. Facilities handling CDC/USDA select agents face additional requirements under 42 CFR Part 73.
How long does BSL-3 laboratory certification take, and how often must it be renewed?
Initial certification requires comprehensive performance testing before first occupancy, typically spanning 4–12 weeks depending on facility complexity. Annual recertification is required and covers airflow performance, pressure differential verification, HEPA filter integrity, and alarm system confirmation.
What HVAC requirements are specific to BSL-3 laboratories?
Core BSL-3 HVAC requirements include:
- Sustained inward directional airflow at all times
- 100% outside air with no recirculation to other building areas
- Continuous pressure differential monitoring at containment barrier entries
- N+1 redundant exhaust fan capacity
- HEPA filtration of exhaust air where required by risk assessment or regulation


